


Must-See Stories & Smart Solutions

The Rosetta Stone of Intelligent Buildings
Does your organization struggle with internal projects because teams aren’t on the same page?
Let's Walk the Talk: Newcomb & Boyd's Sustainability Journey
Newcomb & Boyd’s newly renovated Atlanta Office provides a space that is comfortable, healthy, and sustainable for employees and visitors. Following the company mission and values, the new office incorporates design features focused on sustainability and wellness for employees.


Taking Junction Krog District to LEED Gold
Junction Krog District initially set out to achieve LEED v4 Core and Shell certification at the Certified Level. Through our innovative pilot approaches in energy and water analyses, we gained additional points, surpassing standard documentation pathways. Without incurring any additional costs or requiring extensive design modifications, the collaborative endeavors of our team not only met but exceeded the objective, and the project achieved LEED Gold certification.
Acoustic Modeling
Acoustic modeling services are in high demand, with a range of organizations turning to Newcomb & Boyd and our expert Acoustics teams to help address acoustic challenges.
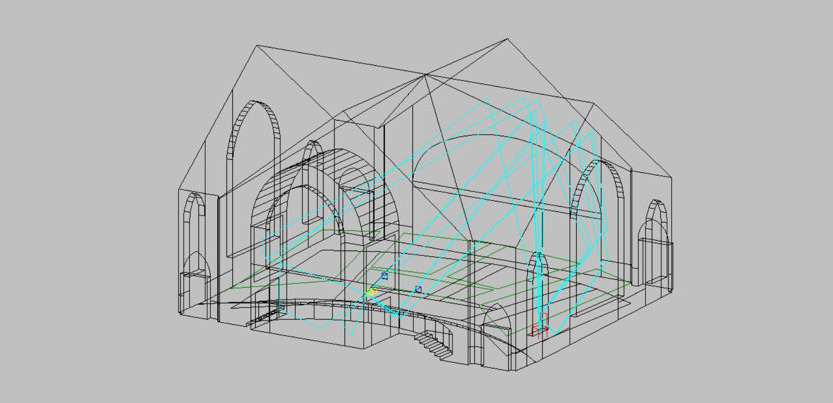
Raytracing
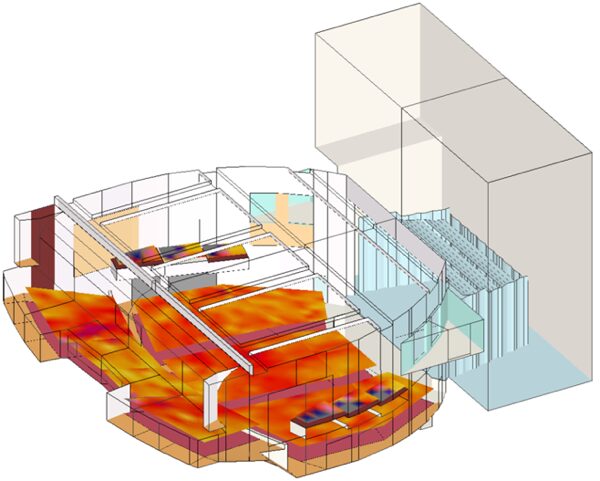
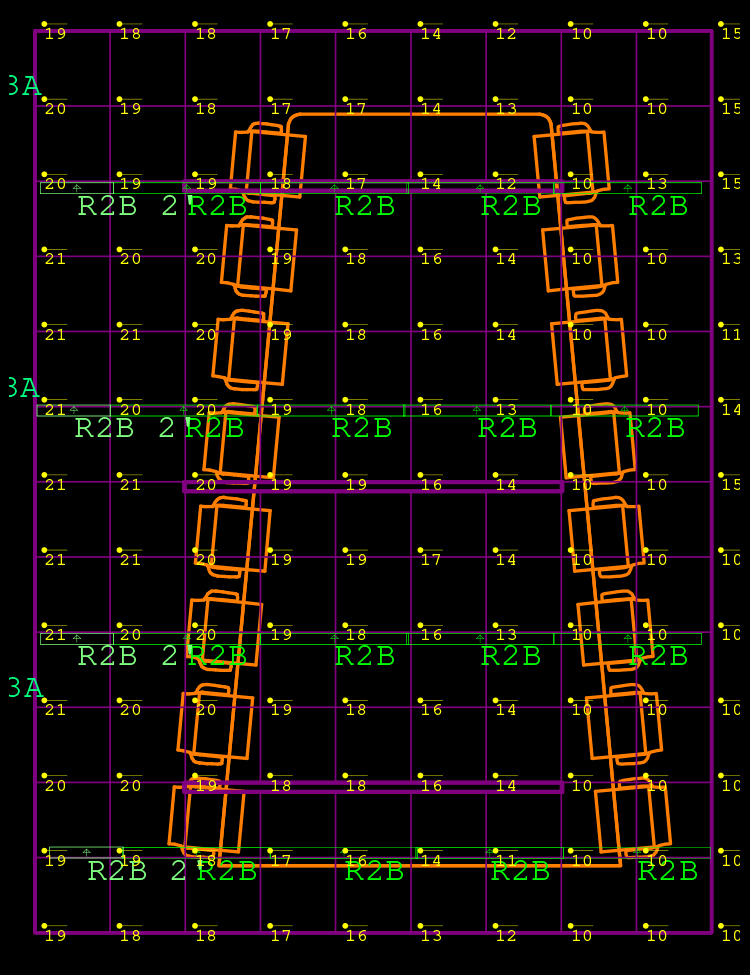
Acoustic Mapping
Through on-site measurements, testing, and analysis we are able to identify acoustic issues and provide solutions that create atmospheres that enhance communication and form a functional, beautiful space.

Invesco's New Headquarters: A Showcase of Innovative Design and Technology
Invesco, a leading global investment management firm, has recently moved into its stunning new headquarters located in the 26-story Midtown Union development in Atlanta. This impressive space represents not just a new office, but a significant leap in design and technology, made possible by Newcomb & Boyd, which provided essential Audiovisual, Telecom, Security, Acoustics, and Specialty Lighting design services.
Cybersecurity Operational Technology Services
Our cybersecurity services offer a comprehensive approach to safeguarding your operational technologies. We enhance cybersecurity awareness through educational programs and create customized frameworks for risk management and asset security. Here’s how we can support you:

Visual Comfort: The Art and Science of Specialty Lighting Design
Did you know that our Specialty Lighting Designers prioritize your visual comfort?
It’s true! We’re dedicated to creating lighting solutions that not only illuminate your spaces but also ensure you can perform tasks comfortably and without strain.
Let’s take a closer look at how we achieve this.
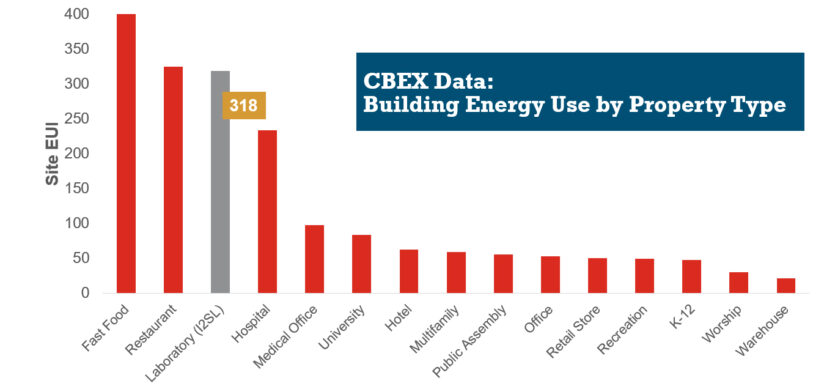
HVAC Design Approaches for Sustainable Laboratories
HVAC systems in a typical laboratory facility can use five to 10 times as much energy as the systems in a typical office building. This higher energy use is due to many factors, including 100 percent outside air systems, 24-hour-a-day operation, high internal heat gains, high air change rate requirements, equipment exhaust requirements, and high fan energy. With this significant energy use, the incentive for creative sustainable design grows—not only to create forward-thinking research spaces, but to maximize a lab’s ROI.